Primary Constipation: An Underlying Mechanism
B. A. SIKIROV
Abstract
Primary (simple) constipation is a consequence of habitual bowel elimination on common toilet seats. A considerable proportion of the population with normal bowel
movement frequency has difficulty emptying their bowels, the principal cause of which is the obstructive nature of the recta-anal angle and its association with the sitting posture normally used in defecation. The only natural defecation posture for a human being is squatting. The alingment /of the recta-anal angle associated with squatting permits smooth bowel elimination. This prevents excessive straining with the potential for resultant damage to the recta-anal region and, possibly, to the colon and other organs. There is no evidence that habitual bowel elimination at a given time each day contributes considerably to the final act of rectal emptying. The natural behavior to empty the bowels in response to a strong defecation reflex alleviates bowel emptying by means of the recta anal inhibitory reflex.
Introduction
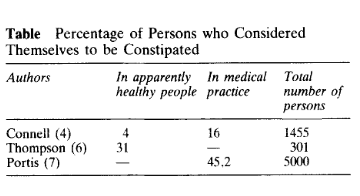
A low frequency of passing stools is the most objective diagnostic sign of constipation (1). Constipation may be considered to be present when a subject has less than three stools per week (2-5). Apart from the fact that only one percent of the normal population has less than three bowel movements per week (4, 5) a significantly greater proportion of normaI subjects considered themselves to be constipated (Table). Why are these people, having normal stool frequency, unsatisfied with their bowel elimination?
Discussion
In a recent trial, a group of 33 patients having normal stool frequency changed their usual habitual bowel emptying from sitting posture to bowel elimination in squatting posture and only in response to urge (8). As a result, patients reported a significant reduction in the amount of straining as expressed in a decreased number of straining episodes. In addition, patient descriptions of the feeling of complete elimination while practicing the squatting posture was in direct contrast to their feelings during habitual defecation on common toilet seats. Historically, man always squatted in order to defecate (9) and the practice continues today in underdeveloped countries (10, 11). The widespread use of toilet seats in Western countries began during the 19th century with the successful development of the water closet and sew age system (12). These technical solutions were necessary for improving sanitary conditions during the growth of cities. As early as the beginning of this century, A. Hurst pointed out that the rise in intraabdominal pressure produced while squatting is, to a great extent, lost when a high seat is used (13). Nearly 50 years later, H. Bockus pointed out that the
ideal position for defecation is the squatting position (14). The accessory muscles that aid in defecation normally have little opportunity to fulfill their function while using common toilet seats. However, only R. E. B. Tagart explained the principal advantage of the squatting defecation posture over the sitting posture (15). He found that the recta-anal angle (at rest SO-900), which is an important factor in anal continence, only slightly straightens out in a common sitting defecation posture.
Maximal straightening out of the recta-anal angle occurs in a squatting posture, thus permitting smooth bowel elimination. Practical means to overcome the difficulties of
bowel elimination arising from the use of an abnormal position were found to be: a) the establishment of a conditional defecation reflex, and b) use of chemical laxatives and bulk producing agents. Establishing a daily routine for defecation at a given time each day, ordinarily in the morning, is a widely accepted prescription for constipated
patients (16, 17). The patient is required to sit on the toilet after breakfast or a glass of water and to stay there for ten minutes or until a stool is passed. The prescription to establish a routine of postprandial bowel movement at a given time each day is based on gastrocolic (11, 18) and conditional (19) reflexes. This is in the hope that
bowel elimination of the subject conditioned to respond to gastro-colic reflex will be alleviated as a result of the increased propulsive activity of the colon. However, the role of peristaltic contraction of the colon in the final act of bowel elimination is unknown (20).
Moreover, the propulsive activity of the colon is insignificant in comparison to expulsive pressures appearing as a result of voluntary straining during defecation (21) and unlikely to contribute considerably to rectal emptying. The routine advice to attempt defecation at a given time each day has an additional drawback. Considering typical western man’s low fiber diet (22), a defecation attempt at a given time each day is associated with low rectal volumes (8, 23). When rectal volumes are low the recta-anal inhibitory reflex is not expressed, consequently, the anal canal is closed due to tonic activity of the anal sphineters (24). As a result bowel emptying requires excessive straining to overcome the resistance of the anal sphineters. Thus, defecation attempts at a given time each day do not facilitate bowel elimination but, in most cases, have quite the opposite effect. The only natural behavior is to empty the bowels in response to a strong defecation reflex. The strong defecation reflex is associated with voluminous rectal quantities that excite the recta-anal inhibitory reflex and result in the relaxation of anal sphinetens, thus facilitating bowel elimination (8, 24). The role of recta-anal inhibitory reflex in alleviation of rectal emptying and reduction of straining is of lesser importance han the factor of alignment of recta-anal angle in squatting posture (8). Patients displaying primary idiopatic constipation with impaired recta-anal sensation and recta-anal inhibitory reflex are probably especially dependent on the unlocking effect of the squatting defecation posture associated with alignment of the rectoanal angle. The use of chemical laxatives and bulk producing agents as a solution for overcoming difficulties related to the abnormal defecation posture is a burdening deviation from normal life.
Conclusion
The principal negative impact of constipation on human health is in its sequelae. For emptying the bowels in a sitting posture, an excessive expulsive effort is needed to overcome resistance of the almost straight recta-anal angle (8, 15). As a result, excessive pressures are generated, which have damaging potential for the recta-anal
region (8, 25) and probably the colon (26) and other organs as well (27). Further research should investigate, by objective methods, the magnitude of expulsive pressures during voluntary straining in the squatting posture versus those in the sitting posture.