MANAGEMENT OF HEMORRHOIDS: A NEW APPROACH
B.A Sikirov
Hemorrhoids are one of mankind's most common ailments (1), but our understanding of the underlying etiologic factors is still insufficient, and treatment, therefore, remains mostly symptomatic and rarely fully successful. Excessive straining during defecation is frequently damaging to the hemorrhoidal venous plexus, anal mucosa and submucosa (2-4). This study undertook to measure the beneficial effect of its diminution. Diminution may be achieved by changing the usual sitting position to a quatting posture (5), and by defecating only in response to a strong urge instead of at a specific time of day (1, 3).
PATIENTS AND METHODS
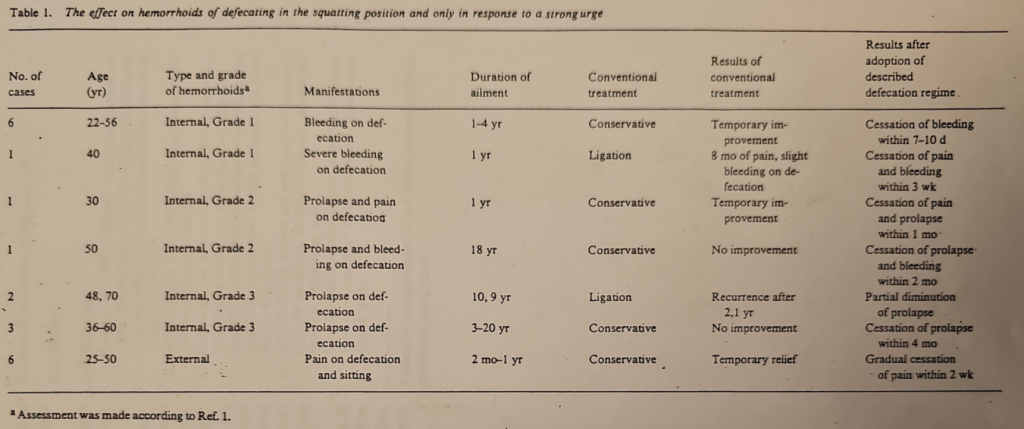
Twenty male and female patients who had hemorrhoids agreed to take part in the study (Table 1). Of these patients, 17 had been undergoing conservative treatments prescribed by their family doctor or surgeon, such as a high fiber diet, suppositories, salves and laxative preparations. The patients had followed the prescribed treatments for a long period of time, and noted only temporary relief. Three patients underwent ligation-two for prolapsed hemorrhoids, with temporary improvement, and one for severe bleeding complicated by severe pains upon attempted defecation. Each patient underwent a thorough proctoscopy and sigmoidoscopy upon inclusion in the study; proctoscopy was repeated after 1 year. In accordance with the above, all 20 patients were asked to modify their defecation habits and postures by 1) defecating in a squatting position only; in order to achieve this position comfortably, and/or in the absence of a squatting lavatory, patients were advised to empty their bowels into any suitable flat container; and 2) defecating only in response to a strong urge to do so; patients were, in fact, advised to postpone the attempt until they were absolutely certain of its necessity.
Results
The results of this study are summarized in Table 1. No abnormal hemorrhoidal swellings were noted during the year following this study, nor were any relapses noted for the year-and-a-half following it, during which time the patients continued to follow the pre- scribed regimen. The two patients who had previously undergone ligation for third-degree internal hemorrhoids, noted only partial diminution of prolapse, and no definite improvement was noted in the follow-up proctoscopy.
Patients who had had external hemorrhoids did not reveal any significant skin tags in the anal region, at the end of the 1-year period.
Discussion
The anatomical advantages of defecating in the squatting posture have been proved in a radiological study (5). The angle between the long axis of the rectum and that of the anal canal is about 80° to 90° in the resting stage (6), and is considered to be one of the important factors of anal continence (1). Tagart (5) has shown that this rectoanal angle slightly straightens when the hips are flexed at 90° and that a maximal straightening of the rectoanal angle occurs when the hips are fully flexed. Thus, a full hip flexion posture decreases resistance at the rectoanal junction, opening the rectoanal outlet and facilitating defecation. More than optimal pressure is employed to propel the fecal mass through the rectoanal canal while defecating in a sitting position. This excessive effort at explusion increases the tendency of the rectoanal mucosa to prolapse, by stretching the mucous membrane. Tagart (5) therefore recommends a squatting position in treating constipation and as a prophylactic measure against hemorrhoids. The habit of emptying the bowels on a regular basis, at a fixed time each day rather than in response to a strong urge, associates with the excessive expulsion effort. A strong defecation reflex occurs when 150 to 200 ml of fecal mass is present in the rectum (7).
The evacuation of feces during an urge obviates excessive straining (1, 3). The habit of emptying the bowels regularly at a fixed time of the day may be associated with a smaller amount of feces in the rectum than needed to evoke an urge. Excessive straining is then needed in order to defecate. In conclusion, the clinical data of this study have shown that excessive straining perpetuates hemor- rhoidal disease. Patients who had suffered from various hemor- rhoidal manifestations changed both their defecation posture (from sitting to squatting) and their timing (from a fixed schedule to defecation on urge only). Both changes reduced straining, thus alleviating the manifestations in most patients. Lack of improvement in the two patients with third-degree internal hemorrhoids, who had previously undergone ligation, may be ascribed to fibrous tissue development in the submucosa as a consequence of the ligation. Upon consideration of the results of this study, it may well be that the toilet in its present form should be modified, to allow defecation in a squatting position, and that a program may be needed to reacquaint man with his natural habits.